

Abstract
Background: although azacitidine (AZA) is an established frontline therapy for HR-MDS, approximately 40% of the patients fail to respond and virtually all of the responders will ultimately relapse. We previously reported the poor outcome of patients who failed AZA treatment for whom a median survival of 6 months is expected (Prebet, J Clin Oncol. 2011;29(24):3322). Overexpression of SMO a member of the hedgehog pathways has been observed in HR-MDS. Preclinical data have shown the activity of hedgehog pathway inhibitors and suggested synergism with Hypomethylating agents (HMA) (Zou, PLoSONE 2015; 10(8):e0136843). To harness potential synergism, we designed an add-on trial in which sonidegib (LDE-225), an oral inhibitor, was added to AZA in patients who failed AZA monotherapy.
Patients and methods:
Eligible patients should have IPSS Int-2 or HR-MDS or AML, (to have 10% to 30% marrow blasts), have received a minimum of 6 cycles of AZA monotherapy and to have failed to achieve a response to AZA (defined as CR, CRi, PR or HI as per IWG criteria) in the absence of marrow progression or have relapsed after achieving a response. Patients were scheduled to receive sonidegib daily from day 1 to 28 of 28-day cycles while continuing on AZA at the maximum previously tolerated dose (ie 50 to 75 mg/m²/d for 5-7 days). Two sonidegib dose levels were evaluated in the phase 1 part of the trial (400 and 800 mg/d) according to a classical 3+3 scheme.
Results:
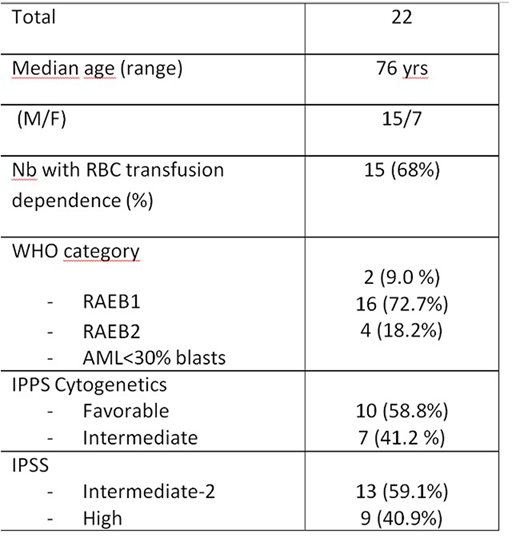
23 patients, median age 76, were included in the study. One withdrew consent before starting the study treatment and is not included in the analysis. Characteristics of the remaining 22 patients are summarized in the Table. At the 800 mg/d dose level, 3 pts experienced DLT (grade 4 ASAT elevation (1 pt); grade 4 CPK elevation (2 pts)). The recommended dose for the expansion phase was 400 mg/d and no DLT was observed. 19 patients received 400 mg/d. Pts received a median of 3.5 cycles [IQR 2 ; 5], and 5 pts (23 %) received ≥ 6 cycles. All of them were withdrawn from study: 5 (26%) for disease progression (including 1 pt who progressed before starting cycle 1 and did not received treatment), 5 (26%) for death (all due to infection in the context of active disease) and 9 for miscellaneous reasons. 25 SAEs were reported including 23 infections, 1 intra cranial hemorrhage and 1 urinary retention. The most frequent non-hematologic toxicity was infection that occurred in 16/22 (73%) pts. In addition, 243 non hematologic toxicities of any grade were recorded in 20 pts for a total of 83 cycles, all but 3 of grade 1-2, including GI, cutaneous and musculo-skeletal toxicities and fatigue. Hospitalization was required in 45% of the pts. Only 3 responses were observed (1 CR, 1 marrow CR and 1 PR). Response durations were 1, 9 and 15 months .With a median follow-up of 23 months, 13 pts have died and the median overall survival is 6.8 months.
Conclusion
Sonidegib at the dose of 400 mg/d can be given in combination with azacitidine with an acceptable toxicity. With a response rate of only 13%, our results indicate that the addition of sonidegib failed to reverse resistance to azacitidine in pts with higher risk MDS. This contrasts with the positive effect of the combination of glasdegib, another hedgehog pathway inhibitor with cytarabine in pts with AML and MDS (Cortes, Blood 2016 128:99). Besides potential differences in drug potency, our results may highlight the difficulty to identify active agents in the difficult-to-treat patient population selected after HMA therapy failure. The recommended dose-schedule of AZA-sonidegib established here could be used for further investigation in previously untreated patients.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal